 Vatsal Khanna
Vatsal Khanna Douglas G. Adler
Douglas G. AdlerIntroduction
Advances in gastrointestinal functional testing have highlighted the limitations of relying on high-resolution manometry (HRM) alone to characterize esophageal pathology, especially with regards to manometric disturbances in patients with dysphagia. While HRM remains the gold standard for evaluating esophageal motor disorders, it provides a pressure-based assessment that may not fully reflect tissue compliance during bolus transit. The functional lumen imaging probe (FLIP) (EndoFLIP developed by Crospon, now Medtronic, Minneapolis, MN, USA) is an impedance planimetry-based technology that provides real-time assessment of luminal geometry and distensibility during volumetric distension.
EndoFLIP serves as an adjunctive diagnostic tool during upper endoscopy to clarify esophageal physiology/pathology when standard testing such as HRM and/or Timed Barium Esophagram (TBE) is inconclusive or discordant with the patient’s symptoms. It is especially helpful in patients with dysphagia, chest pain, or refractory reflux when standard manometry appears normal or equivocal, as FLIP can reveal inadequate esophagogastric junction (EGJ) opening or reduced distensibility that may otherwise be missed.
In addition, EndoFLIP can be used before and after intervention to assess changes in esophagogastric junction opening and distensibility following pneumatic dilation, esophageal or gastric peroral endoscopic myotomy (POEM or G-POEM), laparoscopic Heller myotomy, fundoplication, transoral incisionless fundoplication (TIF), and endoscopic dilation of benign esophageal strictures.
EsoFLIP (Medtronic, Minneapolis, MN, USA) is a therapeutic version of FLIP designed for controlled endoscopic dilation. It uses a stiff, noncompliant balloon that dilates the lumen while measuring diameter in real time. Unlike standard through-the-scope balloons, EsoFLIP allows direct three-dimensional visualization of luminal opening during dilation, adjustment to a target diameter, and dilation without fluoroscopy.
This manuscript summarizes current evidence on EndoFLIP and EsoFLIP with an emphasis on practical indications, clinical interpretation, and recognized limitations. Using common clinical scenarios including Achalasia, Esophagogastric Junction Outlet Obstruction (EGJOO), Esophageal strictures, and anti-reflux or myotomy based therapies, we aim to provide clinicians with a practical guide for applying these technologies in routine clinical practice.
INTRODUCTION
Principle of Impedance
Compliance refers to how easily a hollow organ stretches and increases in volume when pressure is applied, which reflects how well ingested contents can pass through the segment. Impedance planimetry measures this by calculating compliance (volume change relative to pressure) and distensibility (cross-sectional area relative to pressure).1 EndoFLIP was first developed by Hans Gregersen in the 1980s to measure EGJ compliance and distensibility in conditions like GERD and achalasia.,,,
Eventually, in 2009, the first commercially available device of the functional lumen imaging probe (EndoFLIP developed by Crosson, now Medtronic, Minneapolis, MN, USA) was introduced. The EndoFLIP device helps to assess the biomechanical properties of a sphincter or a tubular organ in the gastrointestinal (GI) tract by providing a three-dimensional image of said structure.6 It uses a balloon catheter with impedance electrodes to calculate luminal diameter, cross-sectional area, and distension pressure, allowing for the evaluation of luminal distensibility and compliance. This provides a more detailed understanding of sphincter function compared to HRM and also helps to evaluate esophageal wall stiffness.7
EndoFLIP was initially used to evaluate the EGJ in patients with gastroesophageal reflux disease (GERD) and achalasia.7 Over the past decade, its use has expanded to other esophageal conditions like eosinophilic esophagitis (EOE), and other locations of the GI tract, mostly to the stomach for pylorus measurements in patients with gastroparesis undergoing evaluation and therapy.7 It can also be used before or after foregut procedures (POEM, G-POEM, TIF, surgical myotomy, and fundoplication) to assess treatment response and guide management.6
EsoFLIP (Medtronic, Minneapolis, MN, USA) is a variant of EndoFLIP which combines the advantage of both a diagnostic and a therapeutic tool.6 It is being used as an alternative device for dilation of functional and structural stenoses in the GI tract.6
Technology Overview: What These Tools Actually Measure
EndoFLIP
The EndoFLIP system compromises a 24 cm long catheter with a 3-mm outer diameter and a highly compliant balloon integrated into its tip.7 The catheter is available in two lengths: EF-322 (16 cm) and EF-325 (8 cm).7 The 16 cm catheter consists of 16 electrode pairs spaced 1 cm apart and measures both EGJ metrics and esophageal body contractile response, whereas the 8 cm catheter consists of 16 electrode pairs spaced 0.5 cm apart and primarily measures EGJ metrics.,,,
FLIP measurements utilize impedance planimetry, a technique that is based on Ohm’s Law (voltage is proportional to the impedance which increases with the filling of the balloon) to determine luminal cross-sectional area (CSA), distensibility of the EGJ and/or esophageal body, and esophageal body contractile response to volumetric distention. The equipment consists of a FLIP catheter with impedance planimetry electrodes, and a pressure transducer located inside of polyurethane bag, as well as a digital data acquisition and display system.8
The Dallas Consensus (2025) is an expert statement that standardizes how FLIP panometry is to be performed and interpreted during endoscopy in patients with suspected esophageal motility disorders. This is important because it brings consistency to a test that has been used variably, making FLIP findings easier to interpret and compare across centers.13
EndoFLIP is performed after a standard upper endoscopy to inspect the mucosa and clear luminal contents, typically under monitored anesthesia care (MAC) or general anesthesia.7 The deflated balloon catheter is zeroed to atmospheric pressure and advanced transorally or transnasally into the esophagus or stomach.7 After positioning is confirmed, the balloon is inflated stepwise, starting at 30 mL and increasing in 10 mL increments up to 60 mL for the 16-cm balloon, or from 20 mL up to 50 mL for the 8-cm balloon.7 At each volume, measurements of diameter, cross-sectional area (CSA), intraballoon pressure (IBP), distensibility index (DI), maximum EGJ diameter, and esophageal body contractile pattern are recorded during stable distension for 15–30 seconds to account for respiration and esophageal contractions.7 The balloon is deflated before removal.7
Clinical Indications: When EndoFLIP Adds Value
Use of EndoFLIP in the Esophagus
As per American Gastroenterological Association (AGA) clinical practice update guidelines 2025, clinicians should perform a high-quality upper endoscopy evaluating for esophageal pathology immediately prior to considering FLIP to evaluate for any structural and mucosal abnormalities.8 Physicians should document any visible pathology such as strictures, Eosinophilic Esophagitis (EoE), post operative surgical anatomy, hiatal hernia, as it can impact FLIP catheter placement.,, FLIP can be performed when alternate investigations like HRM or TBE are inconclusive in patients with symptoms of esophageal obstruction such as dysphagia, esophageal-type regurgitation and/or meal-related chest pain.8
Discordance between esophageal test findings is not unusual in patients with symptoms of esophageal dysmotility or dysphagia.8 In a study of 126 symptomatic patients who underwent HRM, TBE, and FLIP, concordance among all the 3 tests assessing lower esophageal sphincter was only 57%. When initial tests are discordant, clinicians should consider using more than one physiologic test to improve diagnostic confidence before proceeding with irreversible lower esophageal sphincter (LES) disruption.,
By measuring distensibility, EndoFLIP helps to diagnose both obstructive and reflux-related processes at the LES and complements the assessment of gastrointestinal motility disorders, particularly achalasia.7
Recent studies involving healthy controls have defined normal EGJ distensibility as EGJ-DI > 2.8 mm2/mm Hg and a maximum EGJ diameter >18 mm. The EGJ opening is described using two parameters, EGJ-DI and maximum EGJ diameter as normal EGJ opening (NEO), reduced EGJ opening (REO), or inconclusive EGJ opening (IEO).13 Esophageal body contractile response patterns can be normal (multiple distinct antegrade contractions and/or repetitive antegrade contractions) or abnormal (absent, diminished, disordered, or spastic contractile response patterns).13 FLIP pressure measurements discriminate diminished ( <40 mm Hg) from disordered ( >40 mm Hg) contractility when distinct antegrade contractions or spastic contractile response are not seen.
Use of FLIP Findings in Making Obstructive Structural and Motor Diagnoses
FLIP panometry aids in distinguishing obstructive structural and motor disorders by combining EGJ opening metrics with esophageal body contractile patterns.8
Normal EGJ opening (EGJ-DI ≥ 2.0 mm²/mm Hg and maximum EGJ diameter ≥ 16 mm) with normal antegrade contractions suggests that a major motor disorder is unlikely.8
Reduced EGJ opening (EGJ-DI < 2.0 mm²/mm Hg and maximum EGJ diameter < 12 mm) supports a structural or motor obstruction in the presence of compatible symptoms and endoscopy findings.8
Absent or weak esophageal contractions, defined as no contractions or a pressure increase < 40 mm Hg, suggest non-spastic achalasia.8 Spastic contractile patterns, such as sustained LES contraction or sustained occluding contractions, are more consistent with spastic achalasia.8 If EGJ opening is reduced but contractility is preserved, a mechanical obstruction should be considered.8
Inconclusive EGJ opening refers to isolated EGJ-DI < 2.0 mm²/mm Hg or a maximum EGJ diameter < 16 mm that does not meet criteria for reduced opening.8 This can be seen with any contractile pattern, and both motor and mechanical obstruction remain possible, requiring further evaluation.8
Role of FLIP in Evaluating Esophageal Motility Disorders
Achalasia
Achalasia is characterized by LES dysfunction and abnormal esophageal peristalsis.7 HRM remains the gold standard test to diagnose achalasia, with EndoFLIP providing supplementary information in some patients.7 HRM has high sensitivity and can identify three distinct achalasia subtypes but may yield inconclusive results in patients with borderline pressure values.7
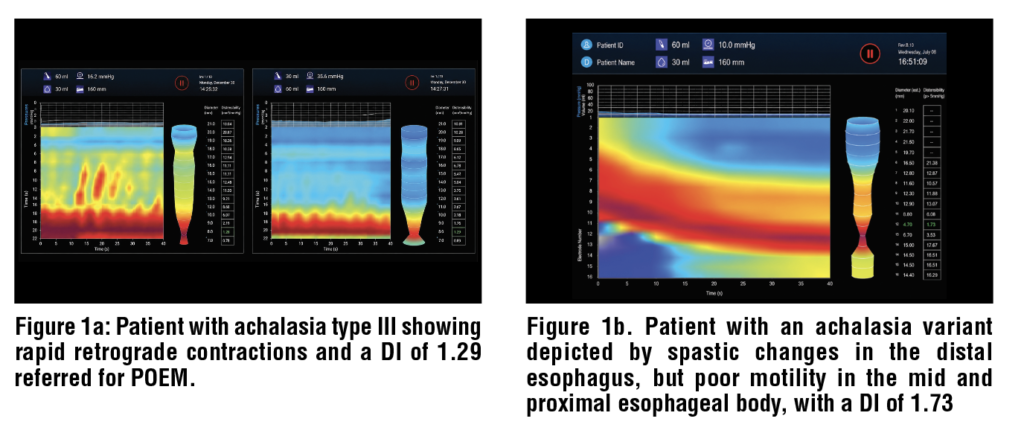
Patients with clinically suspected achalasia who do not meet the HRM criteria of the Chicago Classification v 4.0 (Integrated Relaxation Pressure (IRP) >15 mm Hg in supine position) can be recognized by the FLIP by decreased EGJ-DI or abnormal esophageal contractions., FLIP findings of REO and abnormal contractile response patterns are strongly associated with achalasia.8 (Figure 1)
Endoscopic findings of achalasia are quantified as the CARS (content, anatomy, resistance, and stasis) score. A CARS score ≥ 4 has a specificity of 99% and a sensitivity of 68-72% to identify achalasia. A CARS score of 0-1 combined with NEO on FLIP had a negative predictive value (NPV) of 100% for achalasia and a CARS >4 with REO on FLIP had a positive predictive value(PPV) of 97% for non-spastic achalasia. If upper endoscopy does not demonstrate findings suggestive of achalasia, abnormal EGJ opening on FLIP should prompt further testing with HRM and/or TBE to confirm the diagnosis.8
EGJOO
EndoFLIP plays an important role in evaluating non-achalasia EGJOO.7 EGJOO is a manometric diagnosis with elevated IRP and normal esophageal peristalsis and requires additional testing to confirm EGJ obstruction by either TBE or EndoFLIP to be considered clinically significant.6
In a validation study by Carlson et al., FLIP panometry identified clinically relevant EGJOO in 93% (229/245) of patients when the EGJ-DI was ≥ 3.0 mm²/mm Hg and the maximum EGJ diameter was > 12 mm. These thresholds help to differentiate clinically relevant EGJOO from borderline or incidental findings.27
Role of FLIP in Eosinophilic Esophagitis (EoE)
Eosinophilic esophagitis (EoE) is characterized by chronic immune-mediated inflammation of the esophagus, leading to fibrous changes, stiffening of the esophageal wall with a decrease in esophageal compliance, luminal narrowing, and the formation of strictures., EoE surveillance normally involves upper endoscopy with biopsies and/or dilation as needed to assess histologic activity and guide treatment.
EndoFLIP offers an alternative approach by providing an objective measurement to evaluate esophageal remodeling as well as detection and localization of esophageal narrowing and strictures. EndoFLIP measures esophageal distensibility by recording cross-sectional area and intraluminal pressure during controlled balloon distension.7 This helps to identify the distensibility plateau which corresponds to the luminal opening of the esophagus at its narrowest point.
Patients with EoE have significantly reduced esophageal compliance compared to healthy individuals, with lower distensibility plateaus associated with endoscopic findings such as rings, strictures, increased risk of food impaction and the need for periodic dilation.
The distensibility plateau is defined as a static esophageal diameter despite increasing distention volume and pressure.8 A distensibility plateau of >225 mm2 (diameter > 17 mm) was associated with a lower risk of food impaction and the need for dilation in EoE patients.33 The severity of reduced distensibility plateau correlates with symptom duration and diagnostic delay. In a study by Araujo et al., abnormal esophageal distensibility (≤17 mm) was present in 23% of patients with symptoms for less than 5 years, compared to 64% in those with symptoms for 25 years or more.34 This progressive decline in distensibility supports the concept of EoE as a fibrostenotic disease that worsens over time, particularly in patients with persistent mucosal eosinophilia (≥15 eosinophils per high-powered field).34
Carlson et al. evaluated 215 patients with EoE using FLIP panometry and found abnormal composite measures of esophageal body compliance, contractile response, EGJ distensibility, and maximal diameter were associated with higher eosinophil counts and worse endoscopic severity.
Role of FLIP in Foregut Interventions
Clinicians can consider performing EndoFLIP interprocedurally during myotomy [per-oral endoscopic myotomy (POEM) or laparoscopic Heller Myotomy (LHM)].8
The LES can be evaluated while performing POEM or LHM and can help direct the length of myotomy and adequacy of LES disruption in real time., Intra-operative EGJ-DI <2-3 mm2/mm Hg
may predict persisting symptoms and may prompt additional myotomy.,, In contrast, high intraoperative EGJ-DI may be associated with increased postoperative reflux symptoms, and increase risk of erosive esophagitis after POEM or LHM.,,
Role of FLIP in Symptom Evaluation after Foregut Interventions
Clinicians should consider performing EndoFLIP in patients who have persistent symptoms of esophageal obstruction after treatment of achalasia spectrum disorders by POEM or LHM.8 An EGJ-DI <2-3 mm2/mm Hg after LES disruption is associated with suboptimal esophageal emptying, suggesting ineffective LES disruption, and may warrant consideration of additional LES-directed therapy.,, In contrast, NEO on FLIP should prompt consideration of alternative explanation for symptoms, including abnormal esophageal body anatomy and gastroesophageal reflux disease (GERD).46
FLIP can also be used to assess symptoms after antireflux surgery (ARS), such as fundoplication or bariatric intervention.9 EGJ-DI has been used to tailor fundoplication in attempts to prevent postoperative dysphagia., Tightness of hiatal closure impacts EGJ-DI more than the actual fundoplication. Ideal EGJ-DI ranges have been proposed for Toupet ( EGJ-DI 2.6-3.7 mm2/ mm Hg) and Nissen ( >2.2 mm2/ mm Hg) fundoplication, which helps with intraoperative decision making such as altering the type of ARS, or loosening or tightening the wrap.48
Use of EndoFLIP in the Stomach
Pylorospasm (decreased pyloric distensibility) during gastric contraction plays a key role in the pathophysiology of gastroparesis. Pylorus targeted therapy such as G-POEM can help patients in reducing the symptoms of gastroparesis.6 While EndoFLIP can assess pyloric distensibility, its correlation with gastric emptying and symptoms in gastroparesis remains inconsistent, and the European Society of Gastrointestinal Endoscopy (ESGE) does not currently recommend routine use for pylorus-targeted therapy.
Malik et al. assessed pyloric distensibility in 54 patients with idiopathic and diabetic gastroparesis, the mean distensibility index was 10.7 ± 2.57 mm2/mm Hg, but a wide range of values for both distensibility (1–55 mm2/mm Hg) and diameter (5.6–22.1 mm) was observed. Snape et al. demonstrated that patients presenting with nausea and vomiting and confirmed delayed gastric emptying had decreased pyloric distensibility compared to patients with normal gastric emptying (8 mm2/mm Hg vs. 12.4 mm2/mm Hg). An upper cut-off of 9-10 mm2/mm Hg was used by most of the authors to define pylorospasm while using EndoFLIP.6 Lower pyloric distensibility index in gastroparesis has been linked to better outcomes after G-POEM.
EsoFLIP: The Therapeutic Dilation Catheter
Bougie and balloon dilation are widely used for benign gastrointestinal strictures but provide limited real-time feedback on luminal properties despite endoscopic or fluoroscopic guidance.6 EsoFLIP (Medtronic, Minneapolis, MN) is a more recently developed therapeutic device for esophageal hydraulic balloon dilation and uses the same hardware and technology platform as EndoFLIP, but comes with a stiffer balloon to generate sufficient pressure for dilation.6 The EsoFLIP system offers three catheter sizes: 10 mm (ES-310) and 20 mm (ES-320) balloons for esophageal strictures and a 30 mm (ES-330) balloon, mainly used for patients with achalasia and esophago-gastric junction outflow obstruction.7
Indications for EsoFLIP
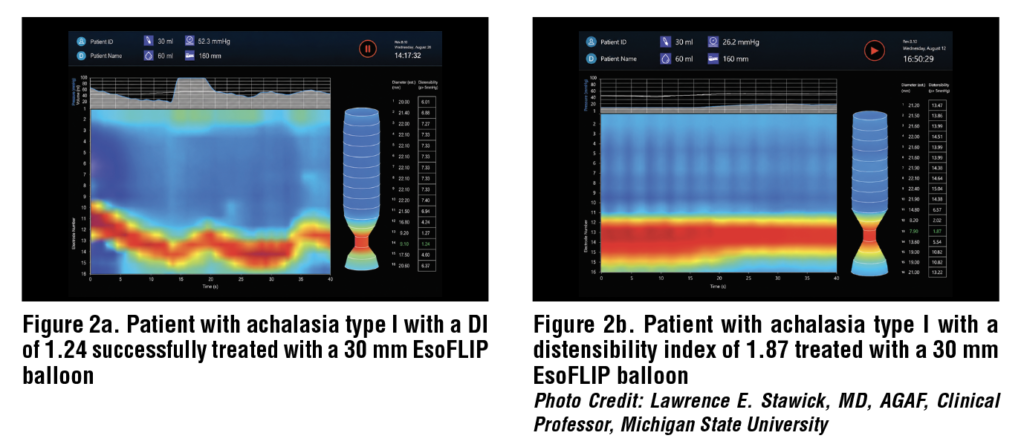
EsoFLIP balloons are used in adults for LES dilation in achalasia and for treatment of esophageal strictures due to surgery, GERD, or radiation as well as the pylorus. (Figure 2)
The inflation of the balloon is manually controlled via an electrohydraulic pump, allowing adjustments based on the target diameter.7 Initial measurements of the diameter or CSA at partial filling volume (20 mL for ES-320 and 30 mL for ES-330) are followed by gradual, stepwise filling to approximately 30 mL/50 mL, with additional increments of 1–3 mL to reach the target diameter. The maximum filling volume of 42 mL/75 mL (ES-320/ES-330) is used to achieve a target diameter of 20-30 mm.7
The advantages of using EsoFLIP over traditional methods of dilation include dilation without the need for fluoroscopy, reducing radiation exposure, precise control of the balloon filling to a desired diameter, and measurement of stricture size and assessment of dilation effect in real time.7 However, these benefits may come at the expense of higher procedural costs.7
Although clinical outcome studies on EsoFLIP are limited, small series have demonstrated its technical feasibility, safety, and short-term efficacy.7 In a feasibility study of 10 patients with achalasia, EsoFLIP achieved dilation to 28–30 mm without serious adverse events with improvement in esophageal symptoms assessed by the Eckardt score as well as improved esophageal emptying recorded with TBE.
Limitations of EndoFLIP and EsoFLIP
EndoFLIP
These include high costs, lack of real-time data processing software, and limited data storage solutions.7 CSA and pressure measurements can vary during stable distension volumes due to respiratory artifacts, vascular effects, and both spontaneous and balloon-induced esophageal contractions. There is limited penetrance outside specialized centers despite commercial availability since 2009, due to lack of data supporting utility in general practice.
EsoFLIP
Although EsoFLIP offers several advantages, it has practical limitations, including lack of through-the-scope capability, the need to remove the external guidewire before dilation, reliance on an external pressure monitor, additional time for balloon filling and emptying, and higher procedural costs.55
Conclusion
The EndoFLIP is an advanced diagnostic tool that helps with the evaluation of sphincters and GI luminal organs by providing real-time dynamic monitoring of distensibility, luminal geometry, and biomechanical properties. It was originally used to assess EGJ, but its application has expanded to other locations including the esophageal body and the pylorus. The device’s ability to measure distensibility can guide the tailoring of specific endoscopic and surgical therapies, such as dilation, fundoplication, and myotomy, to achieve desired outcomes during a single session.
The EsoFLIP is a therapeutic modification of the EndoFLIP catheter that provides real-time visualization and monitoring of dilation as it is being performed via controlled volumetric filling. EsoFLIP represents a useful addition to the treatment of esophageal disorders, although further studies are needed to better define its role and outcomes.
References
1 Wu H, Attaar M, Wong HJ, Campbell M, Kuchta K, Denham
W, Linn J, Ujiki MB. Impedance planimetry (EndoFLIP™)
reveals changes in gastroesophageal junction compliance
during fundoplication. Surg Endosc. 2022 Sep;36(9):6801-
6808. doi: 10.1007/s00464-021-08966-1. Epub 2022 Jan 11.
PMID: 35015103.
2 Gregersen H, Stodkilde-Jorgensen H, Djurhuus JC,
Mortensen SO. The four-electrode impedance technique:
a method for investigation of compliance in luminal
organs. Clin Phys Physiol Meas. 1988;9 Suppl A:61-4. doi:
10.1088/0143-0815/9/4a/011. PMID: 3240652.
3 McMahon BP, Frøkjaer JB, Drewes AM, Gregersen H. A
new measurement of oesophago-gastric junction competence.
Neurogastroenterol Motil. 2004 Oct;16(5):543-6. doi:
10.1111/j.1365-2982.2004.00540.x. PMID: 15500510.
4 McMahon BP, Drewes AM, Gregersen H. Functional oesophago-
gastric junction imaging. World J Gastroenterol. 2006
May 14;12(18):2818-24. doi: 10.3748/wjg.v12.i18.2818.
PMID: 16718804; PMCID: PMC4087796.
5 McMahon BP, Frøkjaer JB, Kunwald P, Liao D, Funch-
Jensen P, Drewes AM, Gregersen H. The functional lumen
imaging probe (FLIP) for evaluation of the esophagogastric
junction. Am J Physiol Gastrointest Liver Physiol. 2007
Jan;292(1): G377-84. doi: 10.1152/ajpgi.00311.2006. Epub
2006 Aug 31. PMID: 16950760.
6 Vackova Z, Levenfus I, Pohl D. Interventional functional
diagnostics in gastrointestinal endoscopy: Combining diagnostic
and therapeutic tools in the endoscopy suite with the
functional lumen imaging probe. Curr Opin Pharmacol. 2023
Dec; 73:102414. doi: 10.1016/j.coph.2023.102414. Epub
2023 Nov 28. PMID: 38029641.
7 Nagl S, Ebigbo A, Messmann H. Use of Endoflip – Impedance
Planimetry System: For Which Indications? Visc Med. 2025
Jun;41(3):137-146. doi: 10.1159/000542545. Epub 2025 Jan
7. PMID: 40519765; PMCID: PMC12165644.
8 Nguyen AD, Carlson DA, Patel A, Gyawali CP. AGA
Clinical Practice Update on Incorporating Functional Lumen
Imaging Probe into Esophageal Clinical Practice: Expert
Review. Gastroenterology. 2025 Sep;169(4):726-736.e1.
doi: 10.1053/j.gastro.2025.05.011. Epub 2025 Jul 18. PMID:
40679455.
9 Kwiatek MA, Kahrilas K, Soper NJ, Bulsiewicz WJ,
McMahon BP, Gregersen H, Pandolfino JE. Esophagogastric
junction distensibility after fundoplication assessed with a
novel functional luminal imaging probe. J Gastrointest Surg.
2010 Feb;14(2):268-76. doi: 10.1007/s11605-009-1086-1.
PMID: 19911238; PMCID: PMC2877633.
10 Rohof WO, Hirsch DP, Kessing BF, Boeckxstaens GE.
Efficacy of treatment for patients with achalasia depends
on the distensibility of the esophagogastric junction.
Gastroenterology. 2012 Aug;143(2):328-35. doi: 10.1053/j.
gastro.2012.04.048. Epub 2012 May 2. PMID: 22562023.
11 Tucker E, Sweis R, Anggiansah A, Wong T, Telakis E,
Knowles K, Wright J, Fox M. Measurement of esophagogastric
junction cross-sectional area and distensibility by an
endolumenal functional lumen imaging probe for the diagnosis
of gastro-esophageal reflux disease. Neurogastroenterol
Motil. 2013 Nov;25(11):904-10. doi: 10.1111/nmo.12218.
Epub 2013 Aug 26. PMID: 23981175.
12 Carlson DA, Lin Z, Rogers MC, Lin CY, Kahrilas PJ,
Pandolfino JE. Utilizing functional lumen imaging probe topography to evaluate esophageal contractility during volumetric
distention: a pilot study. Neurogastroenterol Motil.
2015 Jul;27(7):981-9. doi: 10.1111/nmo.12572. Epub 2015
Apr 20. PMID: 25898916; PMCID: PMC4478241.
13 Carlson DA, Pandolfino JE, Yadlapati R, Vela MF, Spechler
SJ, Schnoll-Sussman FH, Lynch K, Lazarescu A, Khan A,
Katz P, Jain AS, Gyawali CP, Gupta M, Garza JM, Fass R,
Clarke JO, Chokshi RV, Chen J, Ravi K, Chan WW, Sultan
S, Konda VJA. A Standardized Approach to Performing and
Interpreting Functional Lumen Imaging Probe Panometry
for Esophageal Motility Disorders: The Dallas Consensus.
Gastroenterology. 2025 Jun;168(6):1114-1127.e5. doi:
10.1053/j.gastro.2025.01.234. Epub 2025 Feb 4. PMID:
39914779; PMCID: PMC12104001.
14 Kahrilas PJ, Kim HC, Pandolfino JE. Approaches to the
diagnosis and grading of hiatal hernia. Best Pract Res
Clin Gastroenterol. 2008;22(4):601-16. doi: 10.1016/j.
bpg.2007.12.007. PMID: 18656819; PMCID: PMC2548324.
15 Nguyen NT, Thosani NC, Canto MI, et al. The American
Foregut Society White Paper on the Endoscopic Classification
of Esophagogastric Junction Integrity. Foregut: The Journal
of the American Foregut Society. 2022;2(4):339-348.
doi:10.1177/26345161221126961.
16 Jailwala J, Massey B, Staff D, Shaker R, Hogan W. Postfundoplication
symptoms: the role for endoscopic assessment
of fundoplication integrity. Gastrointest Endosc. 2001
Sep;54(3):351-6. doi: 10.1067/mge.2001.117548. PMID:
11522977.
17 Reddy CA, Ellison A, Cipher DJ, Mendoza R, Souza RF,
Spechler SJ, Konda VJA, Nguyen AD. Frequent discrepancies
among diagnostic tests for detecting lower esophageal
sphincter-related obstruction. Neurogastroenterol Motil.
2024 Mar;36(3):e14729. doi: 10.1111/nmo.14729. Epub
2023 Dec 21. PMID: 38129627.
18 Yadlapati R, Kahrilas PJ, Fox MR, Bredenoord AJ, Prakash
Gyawali C, Roman S, Babaei A, Mittal RK, Rommel
N, Savarino E, Sifrim D, Smout A, Vaezi MF, Zerbib
F, Akiyama J, Bhatia S, Bor S, Carlson DA, Chen JW,
Cisternas D, Cock C, Coss-Adame E, de Bortoli N, Defilippi
C, Fass R, Ghoshal UC, Gonlachanvit S, Hani A, Hebbard
GS, Wook Jung K, Katz P, Katzka DA, Khan A, Kohn GP,
Lazarescu A, Lengliner J, Mittal SK, Omari T, Park MI,
Penagini R, Pohl D, Richter JE, Serra J, Sweis R, Tack J,
Tatum RP, Tutuian R, Vela MF, Wong RK, Wu JC, Xiao
Y, Pandolfino JE. Esophageal motility disorders on highresolution
manometry: Chicago classification version 4.0©.
Neurogastroenterol Motil. 2021 Jan;33(1):e14058. doi:
10.1111/nmo.14058. Erratum in: Neurogastroenterol Motil.
2024 Feb;36(2):e14179. doi: 10.1111/nmo.14179. PMID:
33373111; PMCID: PMC8034247.
19 Bredenoord AJ, Babaei A, Carlson D, Omari T, Akiyama J,
Yadlapati R, Pandolfino JE, Richter J, Fass R. Esophagogastric
junction outflow obstruction. Neurogastroenterol Motil.
2021 Sep;33(9):e14193. doi: 10.1111/nmo.14193. Epub
2021 Jun 12. PMID: 34120375.
20 Carlson DA, Kou W, Lin Z, Hinchcliff M, Thakrar A,
Falmagne S, Prescott J, Dorian E, Kahrilas PJ, Pandolfino JE.
Normal Values of Esophageal Distensibility and Distension-
Induced Contractility Measured by Functional Luminal
Imaging Probe Panometry. Clin Gastroenterol Hepatol. 2019
Mar;17(4):674-681.e1. doi: 10.1016/j.cgh.2018.07.042.
Epub 2018 Aug 3. PMID: 30081222; PMCID: PMC6360138.
21 Chambo L, Pandolfino JE, Halder S, Kahrilas PJ, Konda
V, Carlson DA. Discriminating “impaired” from “disordered”
contractile response on FLIP panometry by utilizing
pressure measurement. Neurogastroenterol Motil. 2024
Jul;36(7):e14818. doi: 10.1111/nmo.14818. Epub 2024 May
19. PMID: 38764235.
22 Carlson DA, Lin Z, Kahrilas PJ, Sternbach J, Donnan
EN, Friesen L, Listernick Z, Mogni B, Pandolfino JE.
The Functional Lumen Imaging Probe Detects Esophageal
Contractility Not Observed With Manometry in Patients
With Achalasia. Gastroenterology. 2015 Dec;149(7):1742-
51. doi: 10.1053/j.gastro.2015.08.005. Epub 2015 Aug 14.
PMID: 26278501; PMCID: PMC4663149.
23 Ponds FA, Bredenoord AJ, Kessing BF, Smout AJ.
Esophagogastric junction distensibility identifies achalasia
subgroup with manometrically normal esophagogastric
junction relaxation. Neurogastroenterol Motil. 2017
Jan;29(1). doi: 10.1111/nmo.12908. Epub 2016 Jul 25.
PMID: 27458129.
24 Ellison A, Peller M, Nguyen AD, Carlson DA, Keswani R,
Schauer JM, Reddy CA, Souza RF, Spechler SJ, Pandolfino
JE, Konda VJA. An endoscopic scoring system for achalasia:
the CARS score. Gastrointest Endosc. 2024 Sep;100(3):417-
428.e1. doi: 10.1016/j.gie.2024.02.020. Epub 2024 Feb 29.
PMID: 38431105.
25 Li M, Fass OZ, Carlson DA, Pitisuttithum P, Goudie E,
Kristinsdottir K, Kaklamanos E, Etemadi M, Keswani
RN, Ellison A, Konda VJA, Pandolfino JE. Endoscopic
Prediction of Achalasia: Putting the CART Before the
CARS. Neurogastroenterol Motil. 2025 Jul;37(7):e70024.
doi: 10.1111/nmo.70024. Epub 2025 Mar 17. PMID:
40096578; PMCID: PMC12163212.
26 Carlson DA, Li M, Fass O, Pitisuttithum P, Goudie E, Kou
W, Keswani RN, Pandolfino JE. A combined endoscopy
and functional lumen imaging probe panometry approach
can expedite diagnosis of esophageal motility disorders.
Gastrointest Endosc. 2025 Dec;102(6):811-821.e4. doi:
10.1016/j.gie.2025.03.1329. Epub 2025 Apr 8. PMID:
40210016; PMCID: PMC12354036.
27 Carlson DA, Prescott JE, Baumann AJ, Schauer JM, Krause A,
Donnan EN, Kou W, Kahrilas PJ, Pandolfino JE. Validation of
Clinically Relevant Thresholds of Esophagogastric Junction
Obstruction Using FLIP Panometry. Clin Gastroenterol
Hepatol. 2022 Jun;20(6):e1250-e1262. doi: 10.1016/j.
cgh.2021.06.040. Epub 2021 Jun 30. PMID: 34216821;
PMCID: PMC8716679.
28 Liacouras CA, Furuta GT, Hirano I, Atkins D, Attwood
SE, Bonis PA, Burks AW, Chehade M, Collins MH, Dellon
ES, Dohil R, Falk GW, Gonsalves N, Gupta SK, Katzka
DA, Lucendo AJ, Markowitz JE, Noel RJ, Odze RD,
Putnam PE, Richter JE, Romero Y, Ruchelli E, Sampson
HA, Schoepfer A, Shaheen NJ, Sicherer SH, Spechler S,
Spergel JM, Straumann A, Wershil BK, Rothenberg ME,
Aceves SS. Eosinophilic esophagitis: updated consensus
recommendations for children and adults. J Allergy Clin
Immunol. 2011 Jul;128(1):3-20.e6; quiz 21-2. doi: 10.1016/j.
jaci.2011.02.040. Epub 2011 Apr 7. PMID: 21477849.
29 Schoepfer AM, Safroneeva E, Bussmann C, Kuchen T,
Portmann S, Simon HU, Straumann A. Delay in diagnosis
of eosinophilic esophagitis increases risk for stricture formation
in a time-dependent manner. Gastroenterology. 2013
Dec;145(6):1230-6.e1-2. doi: 10.1053/j.gastro.2013.08.015.
Epub 2013 Aug 13. PMID: 23954315.
30 Dellon ES, Gonsalves N, Hirano I, Furuta GT, Liacouras CA, Katzka DA; American College of Gastroenterology.
ACG clinical guideline: Evidenced based approach to the
diagnosis and management of esophageal eosinophilia and
eosinophilic esophagitis (EoE). Am J Gastroenterol. 2013
May;108(5):679-92; quiz 693. doi: 10.1038/ajg.2013.71.
Epub 2013 Apr 9. PMID: 23567357.
31 Kwiatek MA, Hirano I, Kahrilas PJ, Rothe J, Luger D,
Pandolfino JE. Mechanical properties of the esophagus
in eosinophilic esophagitis. Gastroenterology. 2011
Jan;140(1):82-90. doi: 10.1053/j.gastro.2010.09.037. Epub
2010 Sep 19. PMID: 20858491; PMCID: PMC3008315.
32 Nicodème F, Hirano I, Chen J, Robinson K, Lin Z, Xiao
Y, Gonsalves N, Kwasny MJ, Kahrilas PJ, Pandolfino JE.
Esophageal distensibility as a measure of disease severity
in patients with eosinophilic esophagitis. Clin Gastroenterol
Hepatol. 2013 Sep;11(9):1101-1107.e1. doi: 10.1016/j.
cgh.2013.03.020. Epub 2013 Apr 13. PMID: 23591279;
PMCID: PMC3790569. Nicodème F, Hirano I, Chen J,
Robinson K, Lin Z, Xiao Y, Gonsalves N, Kwasny MJ, Kahrilas
PJ, Pandolfino JE. Esophageal distensibility as a measure of
disease severity in patients with eosinophilic esophagitis.
Clin Gastroenterol Hepatol. 2013 Sep;11(9):1101-1107.e1.
doi: 10.1016/j.cgh.2013.03.020. Epub 2013 Apr 13. PMID:
23591279; PMCID: PMC3790569.
33 Chen JW, Pandolfino JE, Lin Z, Ciolino JD, Gonsalves N,
Kahrilas PJ, Hirano I. Severity of endoscopically identified
esophageal rings correlates with reduced esophageal
distensibility in eosinophilic esophagitis. Endoscopy. 2016
Sep;48(9):794-801. doi: 10.1055/s-0042-107340. Epub 2016
May 20. PMID: 27200524; PMCID: PMC5757503.
34 Araujo IK, Shehata C, Hirano I, Gonsalves N, Kahrilas
PJ, Tetreault MP, Schauer JM, Farina D, Peterson S, Kou
W, Pandolfino JE, Carlson DA. The Severity of Reduced
Esophageal Distensibility Parallels Eosinophilic Esophagitis
Disease Duration. Clin Gastroenterol Hepatol. 2024
Mar;22(3):513-522.e1. doi: 10.1016/j.cgh.2023.04.027. Epub
2023 May 8. PMID: 37164112; PMCID: PMC10630533.
35 Carlson DA, Hirano I, Gonsalves N, Kahrilas PJ, Araujo
IK, Yang M, Tetreault MP, Pandolfino JE. Composite score
of physio mechanical esophageal function using functional
lumen imaging probe panometry in eosinophilic esophagitis.
Gastrointest Endosc. 2024 Apr;99(4):499-510.e1.
doi: 10.1016/j.gie.2023.10.048. Epub 2023 Oct 27. PMID:
37890596; PMCID: PMC11090643.
36 Yang D, Bechara R, Dunst CM, Konda VJA. AGA Clinical
Practice Update on Advances in Per-Oral Endoscopic
Myotomy (POEM) and Remaining Questions-What We
Have Learned in the Past Decade: Expert Review.
Gastroenterology. 2024 Dec;167(7):1483-1490. doi:
10.1053/j.gastro.2024.08.038. Epub 2024 Oct 16. PMID:
39425737.
37 Campagna RAJ, Carlson DA, Hungness ES, Holmstrom
AL, Pandolfino JE, Soper NJ, Teitelbaum EN. Intraoperative
assessment of esophageal motility using FLIP during myotomy
for achalasia. Surg Endosc. 2020 Jun;34(6):2593-
2600. doi: 10.1007/s00464-019-07028-x. Epub 2019 Aug 2.
PMID: 31376012; PMCID: PMC6995437.
38 Teitelbaum EN, Soper NJ, Pandolfino JE, Kahrilas PJ,
Hirano I, Boris L, Nicodème F, Lin Z, Hungness ES.
Esophagogastric junction distensibility measurements during
Heller myotomy and POEM for achalasia predict
postoperative symptomatic outcomes. Surg Endosc. 2015
Mar;29(3):522-8. doi: 10.1007/s00464-014-3733-1. Epub
2014 Jul 24. PMID: 25055891; PMCID: PMC4343529.
39 Ngamruengphong S, von Rahden BH, Filser J, Tyberg A,
Desai A, Sharaiha RZ, Lambroza A, Kumbhari V, El Zein
M, Abdelgelil A, Besharati S, Clarke JO, Stein EM, Kalloo
AN, Kahaleh M, Khashab MA. Intraoperative measurement
of esophagogastric junction cross-sectional area by impedance
planimetry correlates with clinical outcomes of peroral
endoscopic myotomy for achalasia: a multicenter study. Surg
Endosc. 2016 Jul;30(7):2886-94. doi: 10.1007/s00464-015-
4574-2. Epub 2015 Oct 20. PMID: 26487227.
40 Amundson JR, Wu H, VanDruff V, Campbell M, Kuchta K,
Hedberg HM, Ujiki MB. Esophagogastric junction compliance
on impedance planimetry (EndoFLIP™) following
peroral endoscopic myotomy (POEM) predicts improvement
in postoperative eckardt score. Surg Endosc. 2023
Feb;37(2):1493-1500. doi: 10.1007/s00464-022-09432-2.
Epub 2022 Jul 15. PMID: 35838832.
41 Holmstrom AL, Campagna RJ, Carlson DA, Pandolfino
JE, Soper NJ, Hungness ES, Teitelbaum EN. Comparison
of preoperative, intraoperative, and follow-up functional
luminal imaging probe measurements in patients undergoing
myotomy for achalasia. Gastrointest Endosc. 2021
Sep;94(3):509-514. doi: 10.1016/j.gie.2021.02.031. Epub
2021 Mar 1. PMID: 33662363; PMCID: PMC8380635.
42 Eke C, Greenberg I, Bushe B, Joelson A, Acharya P, Lee
D, Sethi A, Kedia P. Utility of Intraprocedural Luminal
Diameter and Distensibility Measurements During the
Esophageal Peroral Endoscopic Myotomy Procedure. J
Clin Gastroenterol. 2024 Nov-Dec 01;58(10):970-974. doi:
10.1097/MCG.0000000000001960. Epub 2024 Jan 15.
PMID: 38227843.
43 Attaar M, Su B, Wong HJ, Kuchta K, Denham W, Haggerty
SP, Linn J, Ujiki MB. Intraoperative impedance planimetry
(EndoFLIP™) results and development of esophagitis in
patients undergoing peroral endoscopic myotomy (POEM).
Surg Endosc. 2021 Aug;35(8):4555-4562. doi: 10.1007/
s00464-020-07876-y. Epub 2020 Aug 13. PMID: 32789722.
44 Rohof WO, Hirsch DP, Kessing BF, Boeckxstaens GE.
Efficacy of treatment for patients with achalasia depends
on the distensibility of the esophagogastric junction.
Gastroenterology. 2012 Aug;143(2):328-35. doi: 10.1053/j.
gastro.2012.04.048. Epub 2012 May 2. PMID: 22562023.
45 Pandolfino JE, de Ruigh A, Nicodème F, Xiao Y, Boris L,
Kahrilas PJ. Distensibility of the esophagogastric junction
assessed with the functional lumen imaging probe
(FLIP™) in achalasia patients. Neurogastroenterol Motil.
2013 Jun;25(6):496-501. doi: 10.1111/nmo.12097. Epub
2013 Feb 17. PMID: 23413801; PMCID: PMC3789137.
46 Jain AS, Carlson DA, Triggs J, Tye M, Kou W, Campagna
R, Hungness E, Kim D, Kahrilas PJ, Pandolfino JE.
Esophagogastric Junction Distensibility on Functional
Lumen Imaging Probe Topography Predicts Treatment
Response in Achalasia-Anatomy Matters! Am J
Gastroenterol. 2019 Sep;114(9):1455-1463. doi: 10.14309/
ajg.0000000000000137. PMID: 30741739; PMCID:
PMC6682473.jai.
47 Hoppo T, McMahon BP, Witteman BP, Kraemer SJ,
O’Rourke RW, Gravesen F, Bouvy ND, Jobe BA. Functional
lumen imaging probe to assess geometric changes in the
esophagogastric junction following endolumenal fundoplication.
J Gastrointest Surg. 2011 Jul;15(7):1112-20. doi:
10.1007/s11605-011-1562-2. Epub 2011 May 20. PMID:
21597882.