 Kate Scarlata
Kate ScarlataIrritable Bowel Syndrome (IBS) is a common gastrointestinal (GI) disorder marked by abdominal pain, bloating, and altered bowel habits. Dietary changes are key to managing symptoms, with the low-FODMAP diet being the most evidence-based approach. Its complexity and restrictiveness, however, can make adherence difficult without guidance from a registered dietitian (RD). Given rising concerns around food-related anxiety and disordered eating in IBS, a shift toward more flexible, individualized dietary strategies is emerging. More research is needed to confirm the long-term outcomes of these less restrictive approaches. This review aims to present the current state of scientific evidence on the use of the low-FODMAP diet for managing IBS, including its three-phase structure and possible application of less restrictive FODMAP diet versions. It also explores the key role of GI expert RDs in the practical implementation of diet therapy, including patient assessment for suitability.
Defining IBS: Symptoms, Prevalence, and Impact
Irritable bowel syndrome (IBS) is a multifactorial and commonly encountered GI disorder, classified as a disorder of gut-brain interaction (DGBI). The Rome IV criteria are used to diagnose IBS and includes presence of recurrent abdominal pain occurring at least once weekly in conjunction with disturbances in bowel habits, including changes in stool frequency and form for the past three months, in the absence of identifiable structural or known biomarkers. IBS occurs 2.5 times more in females than males and symptom onset must have occurred at least 6 months prior to diagnosis.1,2
Prevalence rates vary by country; a recent United States based survey study found that 6.1% met Rome IV IBS criteria,3 while higher rates have been found in low- and middle-income countries, ranging from 6-44%.4 The etiology of IBS has yet to be fully characterized but believed to involve GI motility changes, post-infectious reactivity, visceral hypersensitivity, altered gut-brain interactions, microbiota dysbiosis, small intestinal bacterial overgrowth, food sensitivity, carbohydrate malabsorption, and intestinal inflammation. An acute enteric infection can result in post-infectious IBS, and this represents the most direct risk factor for IBS.5,6
While interest and research are growing to better understand the pathophysiology of IBS to guide treatments, perceived efficacy of current therapies remain limited. Based on survey data, it is evident that many patients with IBS continue to face significant challenges. One survey study revealed that most patients would give up 25% of their remaining life (average 15 years) and 14% would risk a 1/1000 chance of death for a treatment that would relieve IBS symptoms.7 Another survey study revealed patients are willing to accept a 1% risk of sudden death in return for a 99% chance of cure of their symptoms from a medication.8 From a health-related quality of life (HRQOL) impact, patients with IBS had significantly worse HRQOL on selected SF-36 scales than patients with diabetes mellitus and end stage renal disease.9
Table 1. FODMAPs: It’s In The Details
| Acronym | Food Components | Rich FODMAP Sources (examples) |
| F– ermentable | ||
| O-ligosaccharide | Fructans and galacto-oligosaccharides (GOS) | Wheat, barley, rye, onion, garlic, legumes (e.g., beans, lentils, chickpeas), pistachios, cashews |
| D-isaccharide | Lactose | Cow, sheep, and goat milk, ice cream, yogurt |
| M-onosaccharide | Excess fructose | Honey, apple, pear, watermelon |
| A-nd | – | – |
| P-olyols | Sugar alcohols: mannitol, sorbitol, xylitol | celery, stone fruits (e.g., apricot, peach, plum), apple, pear, sugar free gum + mints |
Evolution of Diet as a Therapy in Irritable Bowel Syndrome
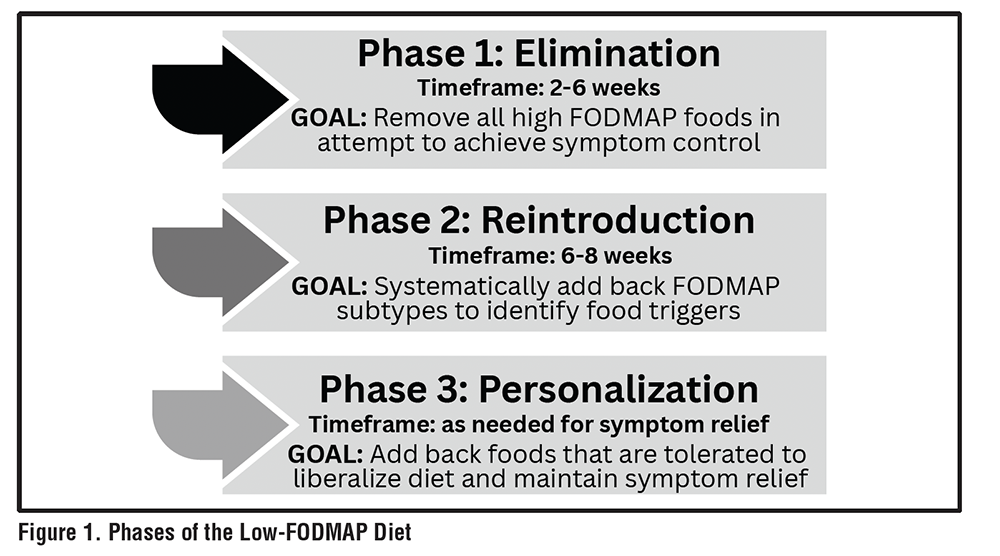
Dietary trials in IBS were limited until the early 2000s. Patients were often prescribed a high fiber diet which offered variable benefits. The term FODMAP (fermentable oligosaccharides, disaccharides, monosaccharides, and polyols) emerged initially in the literature in 2005, speculating a potential link to diet induced small bowel ecology and colonic permeability, potentially predisposing one to inflammatory bowel disease.10 Many individuals living with IBS associate their symptoms to specific foods, which has spurred greater scientific research into the role of diet in managing this challenging and often debilitating disorder. A survey of nearly 200 individuals living with IBS found that 84% believed that eating any food could trigger their symptoms. The majority (70%) identified carbohydrates as triggers, particularly foods rich in fermentable carbohydrates such as dairy products (49%), beans/lentils (36%), apple (28%), flour (24%), and plum (23%).11 See Table 1 for FODMAP subtypes and food sources.The low-FODMAP diet approach evolved into a therapeutic strategy for IBS symptom management, starting initially as a broad elimination diet for IBS, to currently, a three-phase approach. See Figure 1.
Food intolerance (e.g., lactose intolerance) resulting from carbohydrate malabsorption can mimic symptoms of IBS, such as bloating, gas and alteration in bowel habits. The low-FODMAP elimination approach applied a more global restriction to commonly malabsorbed carbohydrates, restricting a wide range of poorly absorbed short-chain carbohydrates. Research trials revealed good efficacy rates, with a notable 50% to 80% of IBS noting clinically relevant symptom benefit.12,13 Efficacy data variability may be due to differences in the approach to diet implementation. In most studies, a dietitian provided guidance on dietary implementation, while participants prepared their own meals. While in the seminal study by Halmos et al., low- FODMAP meals were provided to the participants throughout the study period.14 Currently, there are numerous systematic reviews and meta-analyses supporting the diet’s benefits. A recent systematic and meta-analysis including 15 randomized controlled trials (RCTs) and 1118 participants revealed a benefit over placebo to the low-FODMAP diet, with a risk ratio (RR) of 1.21 (95% confidence interval= 0.98-1.51).15
FODMAP Effect on Gut Physiology in Irritable Bowel Syndrome
As the application of the diet showed benefit globally, further research began to better understand the full mechanism of FODMAPs in IBS. Initial mechanistic insights into how FODMAPs triggered IBS symptoms focused on their effects on luminal distention via osmotic effects and fermentation of the poorly absorbed carbohydrates. This was followed by novel magnetic resonance imaging (MRI) studies that revealed that the size of the FODMAP subtype results in variable effects on bowel distention. The monosaccharide, fructose, distends the small bowel with water due to its greater osmotic effects, while fructans, oligosaccharides, distend the colon from release of gases due to bacterial fermentation.16 The smaller the size of the FODMAP, the greater the osmotic effect while longer chain FODMAP fibers such as fructans, have greater effects on distention via fermentation. In the latest innovative research, investigators using mice models have shown that a high-FODMAP diet may lead to dysbiosis, impaired colonic barrier function, mast cell recruitment and activation, and heightened visceral sensitivity. In mice, a high-FODMAP diet promotes the growth of gram-negative bacteria, resulting in elevated levels of luminal lipopolysaccharide (LPS). This LPS can stimulate mast cells via toll-like receptor 4 (TLR4), triggering the release of bioactive compounds such as tryptase, histamine, and prostaglandin E2. These mediators can, in turn, increase intestinal permeability and enhance visceral sensitivity. Collectively, animal data (and interim analysis from a small human IBS trial) suggests a complex interaction of diet, gut microbiota, immune activation, visceral hypersensitivity and resultant colonic barrier dysfunction.17
A Therapeutic Diet for Irritable Bowel Syndrome: The Low-FODMAP Model
With growing data and research assessing the efficacy of this approach in IBS, the low-FODMAP diet remains the most evidence-based nutritional therapy. The 3-phase approach starts with the elimination phase, followed by the reintroduction phase and lastly the personalization phase. The goal of the elimination phase is to identify FODMAP sensitivity, and if present, alleviate GI symptoms. The next step is to systematically reintroduce FODMAP subtypes back into the diet to identify personal triggers, and lastly, the personalization phase which allows for a more liberal diet, adding back tolerated foods. For those that do not experience any symptom improvement with the elimination phase, the diet should be stopped, and different therapeutic approaches should be explored.
Practical Considerations for Success with the Low FODMAP Diet
Initiating a low-FODMAP diet in an individual with IBS, when possible, should be done under the guidance of a dietitian with expertise in the diet. Research has shown that by applying the diet with dietitian guidance versus without, the patients had a greater likelihood of following the 3-phases appropriately and attaining a therapeutic level of FODMAP intake to effectively reduce symptoms.18 An early referral to a dietitian is important to facilitate accurate and effective implementation of the diet from the outset.
The complexity of the diet benefits from expert RD direction to provide patients with the tools to carry out menu planning, grocery shopping, and label reading to decipher suitable food products for consumption. Further assessment should include considering the patient’s lifestyle, cultural preferences, food accessibility, health literacy, and personal goals for nutrition therapy. Appropriate candidates for the diet are selected carefully through screening for a history of eating disorder or excessive food fear to ensure that a restrictive diet does not induce harm. Using a patient-centered approach is important to confirm the patient desires a nutritional approach to treatment and to gain an understanding on how much they are willing to change in their diet on the onset. See Table 2 for candidates for the low-FODMAP diet.
Table 2. Low-FODMAP Suitability: Clinical Cues and Considerations
| Eating triggers IBS symptoms No eating disorder currently or in past medical history No evidence of heightened food fear Able to prepare own food or have assistance with special diet preparation No signs of malnutrition Desires a nutritional approach |
On the initial visit (generally 45 minutes -1 hour), the RD’s expertise and guidance can reinforce key nutritional principles, including evaluating the patient’s overall dietary adequacy, nutrient balance, eating behaviors (e.g., chewing food thoroughly to maximize digestion, eating in a relaxed state to engage the parasympathetic nervous system for rest and digestion) and promoting a positive, enjoyable relationship with food. While it is essential to encourage mindful adherence to the diet to assess its benefits, care must be taken to avoid fostering hypervigilance. This is particularly important in a population already vulnerable to food-related stress, anxiety and depression due in part to gut-brain axis dysregulation.
Up to one-third of people with IBS also experience anxiety or depression. Individuals with IBS who also experience anxiety or depression may struggle with significant food-related distress. This can include unnecessary and prolonged dietary restrictions, rigid beliefs about certain foods, resistance to altering these beliefs, and fear of eating in situations where they cannot maintain complete control over their diet. For these individuals, it is important to provide clear, evidence-based guidance on appropriate dietary modifications and to dispel common food-related myths. Dietitians can help patients by setting realistic expectations such as noting that diet alone may not resolve GI symptoms and promoting an integrated, multi-disciplinary care approach.19 Integrated care has proven more effective than gastroenterologist-only treatment in improving IBS symptoms, mental health, quality of life, and reducing healthcare costs.20
Figure 2. Top-Down and Bottom-Up Low FODMAP Approach
Potential Downsides of the Low-FODMAP Diet
Stool microbiome analysis research during use of the low-FODMAP diet has highlighted possible adverse effects. During the elimination phase, alterations in the stool microbiome have been observed; however, the potential negative effects of these changes are not yet fully understood. From a gut microbiome impact, the elimination phase of the diet has been shown to increase stool pH, which may provide a more favorable environment for potentially pathogenic microbes to flourish, however this effect is not consistent in the literature.21,22 Further, a reduction in health promoting microbiota, such as bifidobacteria levels are reduced in the elimination phase. However this change has been shown to be mitigated in small clinical trials with use of a probiotic or when the diet is liberalized in the personalization phase.23,24
Nutrient adequacy can be impacted in the elimination phase of the low-FODMAP diet. Diet evaluations of low-FODMAP diet followers appear to be lower in carbohydrates, fiber and calcium.25 It should be noted that in IBS, it is not uncommon for the baseline diet to be nutritionally inadequate. A recent prospective, open-labeled, case-report dietary intervention of 36 patients with IBS showed that an extended low-FODMAP diet (12 weeks) is not inferior to the participants’ baseline diet; revealing the IBS baseline diet has nutrient deficiencies and a low-FODMAP did not exacerbate these.26 The low-FODMAP diet, especially when dietitian-led and appropriately implemented, may be less restrictive than a patient’s baseline diet.
Other concerns about the low-FODMAP diet are its potential impact with food-related quality of life (FRQoL) given its restrictive nature. In fact, finding low-FODMAP suitable food options when dining out can be challenging and the diet requires some level of culinary skills. FRQoL has been found to be reduced in those staying on the elimination phase of the diet versus progressing through the 3 phases.27 Additionally, the potential added costs of following a specialized diet may add another barrier. Low-FODMAP and gluten free products often come at a higher cost compared to traditional wheat-based staples.28
Reintroduction Trials: What Have We Learned
Two trials focused on reintroducing FODMAPs were conducted to determine which FODMAP subtypes are most linked to digestive symptoms in patients with IBS. In one trial, US researchers Eswaran and colleagues carried out a key single-center study to evaluate the effects of reintroducing specific FODMAPs in patients who met the Rome IV criteria for IBS who had shown symptom improvement on a low-FODMAP elimination diet. This small, randomized, double-blind trial involved reintroducing individual FODMAP subtypes, with a final analysis including 20 participants. While maintaining the elimination phase of the low-FODMAP diet, each participant was randomized to follow one of five sequences involving the reintroduction of fructans, excess fructose, galacto-oligosaccharides (GOS), lactose, or polyols, all provided in a brownie. Participants consumed two brownies daily. See Table 3 for reintroduction FODMAP subtype amounts. The study aimed to identify which specific FODMAPs triggered symptoms such as abdominal pain and bloating. Results showed that fructans and GOS were the most common triggers, causing significant increases in abdominal pain, with GOS also linked to increased bloating. In contrast, lactose, excess fructose, and polyols did not significantly affect symptoms. These findings indicate that not all FODMAPs contribute equally to IBS symptoms, supporting a more targeted dietary management approach.29
Table 3. Reintroduction of FODMAP Quantities Administered Each Week29
| FODMAP | Moderate Dose (day 1-3) | High Dose (day 4-7) |
| Lactose | 10 g/day | 20 g/day |
| Excess fructose | 10.5 g/day | 21 g/day |
| Polyol (sorbitol) | 5 g/day | 10 g/day |
| Fructans | 0.75 g/day | 1.5 g/day |
| GOS (galacto-oligosaccharides) | 2 g/day | 4 g/day |
In another reintroduction FODMAP diet trial, Belgium researchers, Van den Houte et al. (2024) provides further validation that not all FODMAP subtypes trigger symptoms in most patients with IBS. Their blinded, randomized, crossover trial aimed to identify specific FODMAP triggers and assess their impact on IBS symptoms, quality of life, and psychosocial comorbidities. In this trial, 117 participants with IBS meeting Rome IV criteria who responded favorably to the low-FODMAP elimination diet phase, defined as a reduction of ≥50 points from baseline on the IBS Severity Scoring System (IBS-SSS), progressed to a 9-week reintroduction phase. During this phase, participants continued the low-FODMAP diet while being exposed to six different FODMAPs or glucose (30 g dose/day) as a control. Each FODMAP was provided as a powdered supplement in a randomized, blinded, crossover sequence. See the daily dosages of FODMAP subtypes are outlined in Table 4. Symptom severity was recorded daily using a 0–10 point numerical rating scale. Symptom recurrence was triggered in 85% of the FODMAP powders, by an average of 2.5 ± 2 FODMAPs/patient. The most prevalent triggers were fructans (56%), mannitol (54%), and GOS (35%).30
Table 4. Daily FODMAP Subtypes and Quantities Tested30
| FODMAPs | Daily Powder Dose |
| Fructans | 20 g/day |
| Excess fructose | 60 g/day |
| GOS | 12 g/day |
| Lactose | 60 g/day |
| Mannitol | 15 g/day |
| Sorbitol | 15 g/day |
These findings sparked interest in the clinical feasibility of achieving adequate symptom control through a more liberal FODMAP restriction.
Variations of the FODMAP Diet
FODMAP Simple
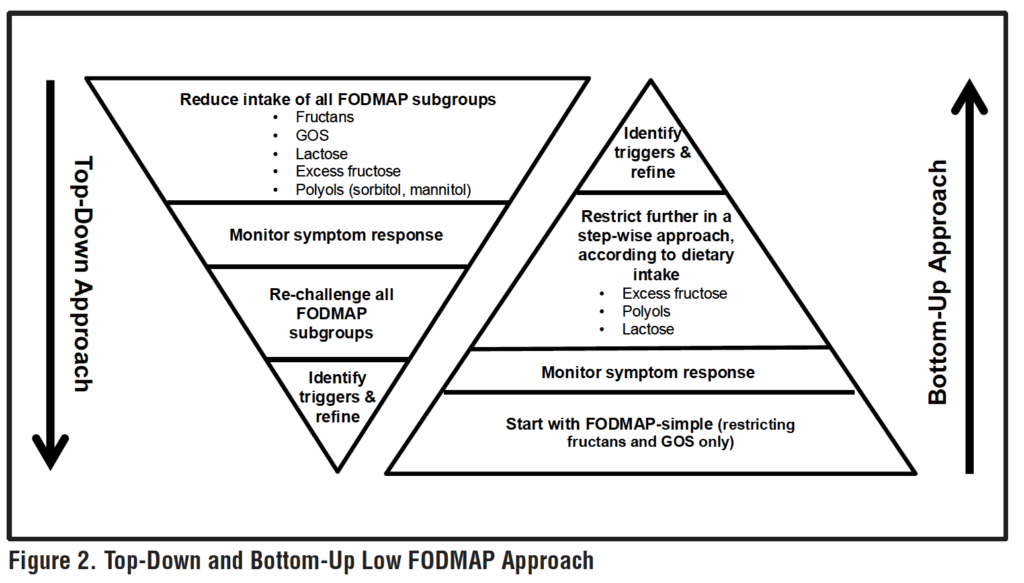
Based on the findings that fructans and GOS are commonly found to be triggers in clinical practice, and both reintroduction studies suggested their common role in instigating symptoms, a 2-center pilot feasibility study was initiated to assess for benefit of a bottom-up approach to FODMAP restriction. The “FODMAP simple” diet only limited fructans and GOS and was compared to the traditional low-FODMAP elimination diet in patients with IBS-with diarrhea (IBS-D). See Figure 2. The pilot feasibility study, which included 10 participants following the traditional low FODMAP diet group and 14 following the FODMAP simple diet, revealed the FODMAP simple approach improved symptoms in majority of patients with IBS-D. Furthermore, the FODMAP simple diet was better tolerated than the traditional low-FODMAP diet (adverse effects rate 12.5% vs. 26.3%).31 Given this was a pilot-feasibility study, the results should be viewed primarily as hypothesis generating versus evidence-based data. While this is not robust data to change clinical practice guidelines, it does provide some signals that a less restrictive approach may be effective for many with IBS.
FODMAP Gentle
In the FODMAP gentle approach, the dietitian modifies FODMAP intake based on the patient’s current intake and symptom profile, identifying only a subset of FODMAP rich foods to eliminate and assess symptom benefit. A FODMAP gentle diet involves selectively reducing certain foods that are highest in FODMAPs. See Table 5 for high-FODMAP foods often excluded in the FODMAP gentle diet.
This approach was introduced by Halmos and Gibson, Monash University researchers suggesting a FODMAP gentle approach may be undertaken when the traditional low-FODMAP elimination diet a “top-down” approach to treatment may not be appropriate.32 The authors highlight that some patients may be more appropriate for a less restrictive form of modifying FODMAPs such as individuals with pre-existing dietary restrictions (e.g., celiac disease, allergies) that may face nutritional deficiencies or those with active eating disorders or with food fear where a highly restrictive diet may exacerbate their psychological and potentially physical health. In such cases, it may be more appropriate to either forgo dietary therapy altogether or adopt a “bottom-up” strategy, such as the FODMAP gentle, a milder form of FODMAP restriction. It’s important to note that the FODMAP gentle approach has not been formally evaluated in the research setting.
Case Vignette:
A Targeted FODMAP Gentle Strategy in Practice
A 23-year-old female with a history of IBS-C (IBS with constipation) presents with an increase in gas and bloating, which she finds increasingly frustrating. She has no history of an eating disorder or noted elevation of food fears. Her weight is stable with no alarm signs (e.g., blood in stool, unintended weight loss). She just started a new job at a coffee shop two months ago, where she has been consuming three complimentary soy lattes per shift as part of her employee benefits. While her constipation improved, symptoms of abdominal pain and gas have increased, which she describes as moderate and impacting on her day-to-day living. During the initial consultation, the dietitian recommended a FODMAP gentle approach, restricting her soy milk (a common source of the FODMAP subtype, GOS). The patient was instructed to substitute with almond milk or lactose free cow’s milk in her lattes. This slight change provided adequate symptom relief for this patient—and no further diet modifications were needed.
Caution: Diet is Not Always a Benign Intervention in Patients with GI Disorders
While often viewed as a holistic and natural approach to IBS care, diet change in the GI patient population may come with some unintended consequences. Of great interest and concern is the association of disordered eating particularly in the face of food fear, or a condition called avoidant restrictive food intake disorder (ARFID). ARFID was first included in the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition in 2013, with a proposed subgroup highlighted by a pathologic restriction resulting from a fear of negative effects associated with eating.33 Further, individuals with past or a current eating disorder (ED) may develop GI symptoms as a consequence from their disordered eating behaviors. Malnutrition, for instance, can lead to pelvic floor dysfunction due to muscle atrophy, a predictor of abdominal distention and constipation.34 It can be challenging to determine whether GI symptoms are intrinsic features of EDs or consequences of malnutrition resulting from behaviors such as laxative misuse, self-induced vomiting, or food restriction.
Table 5. FODMAP Rich Foods Excluded in the Gentle Low-FODMAP Diet
| Food Group | Common High-FODMAP Sources |
| Grains | Wheat, rye |
| Vegetables | Onion, leek, cauliflower, mushrooms (button) |
| Fruit | Apple, pear, dried fruit, stone fruit, watermelon |
| Dairy | Lactose containing milk or yogurt |
| Protein | Legumes (e.g., beans, lentils, chickpeas) |
Healthcare providers in GI are indeed faced with a patient population at risk for disordered eating. One systematic review and meta-analysis found 23.4%of patients with GI disease (n=691) displayed disordered eating patterns.35 Screening for food fear (Nine Item Avoidant/Restrictive Food Intake Disorder Screen (NIAS)) or eating disorders (Eating Attitudes (EAT-26)) can help assess for maladaptive eating behaviors.36,37 With a positive screening for ARFID or ED, a referral to an ED therapist for a clinical diagnosis and management would be the next step.34,38 It is important to note, there is a need for validated ARFID and ED screening tools in the GI patient population. The NIAS can be used to screen for ARFID among patients with IBS; however, the IBS patient population is different than the population NIAS was developed in, and the validity is a bit unclear.37,38 While disordered eating behaviors benefit from eating disorder expert care, it’s important a GI provider remain engaged in GI care as needed.38
Conclusion
The low-FODMAP diet has emerged as a valuable therapeutic tool for managing IBS, offering symptom relief through strategic carbohydrate restriction. It’s complexity and restrictive nature underscore the critical role of GI-Expert RDs in guiding patients through its phases, ensuring nutritional adequacy, helping guide a positive food relationship and mitigating any potential nutrient and diet related health risks. There is growing interest and initial research underway into less restrictive approaches to the low-FODMAP diet, such as “FODMAP Gentle” and “FODMAP Simple”. Given the increasing concern that elimination diets may lead to disordered eating patterns or worsen conditions such as ARFID, especially among GI patients, the aim is to offer individuals with IBS a personalized and as liberal a diet as possible, while still effectively managing symptoms. Ideally, this approach should be initiated and monitored by a qualified GI-expert RD whenever feasible.
References
1. Lacy BE, Pimentel M, Brenner DM, et al. ACG Clinical Guideline:
Management of Irritable Bowel Syndrome. Am J Gastroenterol.
2021;116(1):17-44.
2. Ford AC, Lacy BE, Talley NJ. Irritable bowel syndrome. N Eng J
Med 2017; 376:2566–78.
3. Almario CV, Sharabi E, Chey WD, Lauzon M, Higgins CS, Spiegel
BMR. Prevalence and Burden of Illness of Rome IV Irritable
Bowel Syndrome in the United States: Results from a Nationwide
Cross-Sectional Study. Gastroenterology. 2023;165(6):1475-1487.
4. Arnaout AY, Nerabani Y, Douba Z, Kassem LH, Arnaout K,
Shabouk MB, Zayat H, Mayo W, Bezo Y, Arnaout I, Yousef A,
Zeina MB, Aljarad Z; PRIBS Study Team. The prevalence and risk
factors of irritable bowel syndrome (PRIBS study) among adults in
low- and middle-income countries: A multicenter cross-sectional
study. Health Sci Rep. 2023 Oct 4;6(10): e1592.
5. Tang HY, Jiang AJ, Wang XY, et al. Uncovering the pathophysiology
of irritable bowel syndrome by exploring the gut-brain axis: a
narrative review. Ann Transl Med. 2021;9(14):1187.
6. Ford AC, Sperber AD, Corsetti M, Camilleri M. Irritable bowel
syndrome. Lancet. 2020;396(10263):1675-1688.
7. Drossman DA, Morris CB, Schneck S, et al. international survey
of patients with IBS: Symptom features and their severity, health
status, treatments, and risk Taking to achieve clinical benefit. J
Clin Gastroenterol 2009;43(6):541–50.
8. Lacy BE, Everhart KK, Weiser KT, et al. IBS patients’ willingness to
take risks with medications. Am J Gastroenterol 2012; 107: 804-9.
9. Gralnek IM, Hays RD, Kilbourne A, Naliboff B, Mayer EA. The
impact of irritable bowel syndrome on health-related quality of
life. Gastroenterology. 2000;119(3):654-660.
10. Gibson PR, Shepherd SJ. Personal view: food for thought–western
lifestyle and susceptibility to Crohn’s disease. The FODMAP
hypothesis. Aliment. Pharmacol. Ther. 2005; 21: 1399–1409.
11. Böhn L, Störsrud S, Törnblom H, Bengtsson U, Simrén M.
Self-reported food-related gastrointestinal symptoms in IBS are
common and associated with more severe symptoms and reduced
quality of life. Am J Gastroenterol. 2013;108(5):634-641.
12. Eswaran SL, Chey WD, Han-Markey T, Ball S, Jackson K. A
Randomized Controlled Trial Comparing the Low FODMAP Diet
vs. Modified NICE Guidelines in US Adults with IBS-D. Am J
Gastroenterol. 2016;111(12):1824-1832.
13. Staudacher HM, Whelan K. The low FODMAP diet: recent
advances in understanding its mechanisms and efficacy in
IBS. Gut. 2017;66(8):1517-1527.
14. Halmos EP, Power VA, Shepherd SJ, Gibson PR, Muir JG. A
diet low in FODMAPs reduces symptoms of irritable bowel syndrome.
Gastroenterology. 2014;146(1):67-75. e5.
15. Khan Z, Muhammad SA, Amin MS, Gul A. The Efficacy of the
Low-FODMAP (Fermentable Oligosaccharides, Disaccharides,
Monosaccharides, and Polyols) Diet in Irritable Bowel Syndrome:
A Systematic Review and Meta-Analysis. Cureus. 2025 Jan
7;17(1): e77053.
16. Murray K, Wilkinson-Smith V, Hoad C, et al. Differential effects
of FODMAPs (fermentable oligo-, di-, monosaccharides and
polyols) on small and large intestinal contents in healthy subjects
shown by MRI. Am J Gastroenterol 2014; 109:110–9
17. Singh P, Grabauskas G, Zhou SY, Gao J, Zhang Y, Owyang C.
High FODMAP diet causes barrier loss via lipopolysaccharidemediated
mast cell activation. JCI Insight. 2021 Nov 22;6(22):
e146529.
18. Tuck CJ, Reed DE, Muir JG, Vanner SJ. Implementation of the low
practicalgastro.com FODMAP diet in functional gastrointestinal symptoms: A real-world experience. Neurogastroenterol Motil. 2020;32(1): e13730.
19. Staudacher HM, Black CJ, Teasdale SB, Mikocka-Walus A, Keefer
L. Irritable bowel syndrome and mental health comorbidity –
approach to multidisciplinary management. Nat Rev Gastroenterol
Hepatol. 2023 Sep;20(9):582-596.
20. Basnayake C, Kamm MA, Stanley A, et al. Standard gastroenterologist
versus multidisciplinary treatment for functional
gastrointestinal disorders (MANTRA): an open-label, singlecentre,
randomised controlled trial. Lancet Gastroenterol Hepatol.
2020;5(10):890-899.
21. Halmos EP, Christophersen CT, Bird AR, Shepherd SJ, Gibson
PR, Muir JG. Diets that differ in their FODMAP content alter the
colonic luminal microenvironment. Gut. 2015;64(1):93-100.
22. So D, Loughman A, Staudacher HM. Effects of a low FODMAP
diet on the colonic microbiome in irritable bowel syndrome:
a systematic review with meta-analysis. Am J Clin Nutr.
2022;116(4):943-952.
23. Staudacher HM, Lomer MCE, Farquharson FM, et al. A Diet Low
in FODMAPs Reduces Symptoms in Patients with Irritable Bowel
Syndrome and A Probiotic Restores Bifidobacterium Species: A
Randomized Controlled Trial. Gastroenterology. 2017;153(4):936-
947.
24. Staudacher HM, Rossi M, Kaminski T, et al. Long-term personalized
low FODMAP diet improves symptoms and maintains
luminal Bifidobacteria abundance in irritable bowel
syndrome. Neurogastroenterol Motil. 2022;34(4): e14241.
25. Staudacher HM. Nutritional, microbiological and psychosocial
implications of the low FODMAP diet. J Gastroenterol Hepatol.
2017;32 Suppl 1:16-19.
26. Hillestad EMR, Steinsvik EK, Teige ES, et al. Nutritional safety
and status following a 12-week strict low FODMAP diet in
patients with irritable bowel syndrome. Neurogastroenterol Motil.
2024;36(7):e14814.
27. Silva H, Porter J, Barrett J, Gibson PR, Garg M. Dietary Intake,
Symptom Control and Quality of Life After Dietitian-Delivered
Education on a FODMAP Diet for Irritable Bowel Syndrome: A
7-Year Follow Up. Neurogastroenterol Motil. Published online
July 1, 2025.
28. Lee AR, Wolf RL, Lebwohl B, Ciaccio EJ, Green PHR.
Persistent Economic Burden of the Gluten Free Diet. Nutrients.
2019;11(2):399.
29. Eswaran S, Jencks KJ, Singh P, Rifkin S, Han-Markey T,
Chey WD. All FODMAPs Aren’t Created Equal: Results of a
Randomized Reintroduction Trial in Patients With Irritable Bowel
Syndrome. Clin Gastroenterol Hepatol. 2025;23(2):351-358.e5.
30. Van den Houte K, Colomier E, Routhiaux K, et al. Efficacy and
Findings of a Blinded Randomized Reintroduction Phase for the Low
FODMAP Diet in Irritable Bowel Syndrome. Gastroenterology.
2024;167(2):333-342.
31. Singh P, Chey SW, Nee J, et al. Is a Simplified, Less Restrictive
Low FODMAP Diet Possible? Results From a Double-Blind,
Pilot Randomized Controlled Trial. Clin Gastroenterol Hepatol.
2025;23(2):362-364.e2.
32. Halmos EP, Gibson PR. Controversies and reality of the FODMAP
diet for patients with irritable bowel syndrome. J Gastroenterol
Hepatol. 2019;34(7):1134-1142.
33. American Psychiatric Association. (2013). Diagnostic and
Statistical Manual of Mental Disorders (5th ed.; DSM-5).
Arlington, VA: American Psychiatric Publishing.
34. Riehl ME, Scarlata K. Understanding Disordered Eating Risks
in Patients with Gastrointestinal Conditions. J Acad Nutr Diet.
2022;122(3):491-499.
35. Satherley R, Howard R, Higgs S. Disordered eating practices in
gastrointestinal disorders. Appetite. 2015; 84:240-250.
36. Garner DM, Olmsted MP, Bohr Y, Garfinkel PE. The eating attitudes
test: psychometric features and clinical correlates. Psychol
Med. 1982;12(4):871-878.
37. Zickgraf HF, Ellis JM. Initial validation of the Nine Item Avoidant/
Restrictive Food Intake disorder screen (NIAS): A measure of
three restrictive eating patterns. Appetite. 2018; 123:32-42.
38. Scarlata K, Zickgraf HF, Satherley RM, et al. A Call to Action:
Unraveling the Nuance of Adapted Eating Behaviors in Individuals
with Gastrointestinal Conditions. Clin Gastroenterol Hepatol.
2025;23(6):893-901.e2.